Snapping Scapula Syndrome
Dr.Senthilvelan
Consultant Orthopaedic Surgeon
Anatomy of Scapulothoracic Joint
The scapula is a large, flat, triangular bone that lies along the posterior surface of the thoracic cage between the second and seventh ribs. The scapula is part of the superior shoulder suspensory complex, which provides attachments to the axial skeleton.
The articulation between the scapula and the thoracic cage is one of the most incongruent in the human body. The Scapulothoracic pseudo joint has three layers: superficial, intermediate, and deep layers.
The trapezial bursa lies between the trapezius muscle and the base of the scapular spine and averages 4.3 · 2.7 cm in size. This bursa is particularly important as it provides a smooth surface over which the scapula rotates.
Scapulohumeral rhythm
Scapular control is essential to Scapulohumeral coordination. Posterior tilting is responsible for humeral clearance during the acromio humeral portion of shoulder elevation. Scapular upward rotation and retraction are greatest during abduction, elevation when compared to flexion, elevation. Any disturbance in this rhythm can decrease this Scapulothoracic movement and can be associated with fatigue, impingement, and instability and limits elevation.
Pathophysiology of Snapping Scapula Syndrome
Scapulothoracic motion produces a snapping, grinding or popping sensation. There are many causes to produce crepitus ranging from repetitive forceful shoulder movements producing microtrauma , resulting in a bone spur at the muscular attachment on scapula, to crepitus that can be a end result of bursitis.
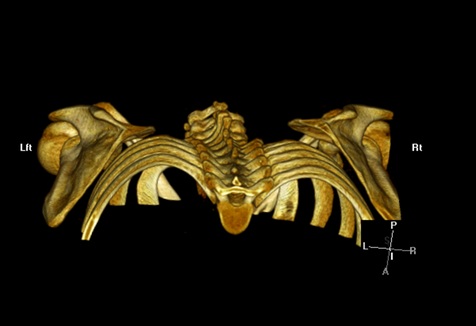 |
| 3D CT showing decreased Scapulothoracic distance on left side. |
Approximately 6% of scapulae demonstrate a hook-shaped prominence, known as
the Luschka tubercle, at their superomedial angle. This tubercle may enlarge and articulate with the thoracic cage, resulting in painful crepitus. However, a clear causal relationship between
this morphology and the presence of scapulothoracic bursitis has not been demonstrated.
 |
| CT scan showing Lushkas Tubercle |
Osteochondroma is the most prevalent benign tumor of the scapula and has been implicated as a common cause of snapping scapula syndrome. Scapulothoracic bursitis may also occur following loss of dynamic control of scapular motion.
Muscle atrophy secondary to nerve injury, trauma, or prior operative treatment can lead to diminished soft-tissue interposition between the scapula and the thoracic cage, resulting in scapulothoracic crepitus and pain.
Management
Non operative management
The majority of patients with scapulothoracic crepitus or bursitis can be managed successfully without operative treatment. Operative management may be considered for patients who
have undergone a prolonged course of nonoperative treatment with little or no improvement.
Arthroscopic Surgery
Arthroscopic surgery for snapping scapula syndrome offers several theoretical advantages over open operative treatment. These include minimizing dissection and preserving muscle attachments, thereby eliminating the need for postoperative immobilization and potentially shortening the rehabilitation period.
Other advantages include an improved cosmetic appearance and potentially decreased hospital stays.
Technique of arthroscopic Surgery
The patient is positioned prone with the arm extended and internally rotated to accentuate the medial border of the scapula. All standard portals are established at least 3 cm
medial to the medial border of the scapula to avoid injuring the dorsal scapular nerve and vessels.
 |
| Patient is positioned Prone for Scapulothoracic Bursoscopy |
Along the vertical axis, the superior visualization portal is placed just inferior to
the scapular spine to allow access to both the superomedial and the inferomedial angle of the scapula.
Under arthroscopic visualization, the inferior working portal is then created midway between the scapular spine and the inferomedial scapular angle. The instruments are pointed away from the coracoid process to prevent damage to the suprascapular nerve and vessels, which travel just medial to the base of the coracoid.
The visualization and working portals may be interchanged as needed intraoperatively for improved access to the bursal tissues. Portals placed superior to the scapular spine may result in injury to the dorsal scapular nerve and vessels or the spinal accessory nerve, and is avoided.
Intially scapulothorcic bursectomy is completed,and then subsequently the arm is moved under direct visualization and if the superomedial angle is deemed prominent a partial scapular resection is performed.
Before the procedure is completed, the scapulothoracic joint is examined with the patient under anesthesia to ensure that no impinging structures remain.
An advantage to arthroscopic debridement is that the periosteal sleeve of the rhomboid attachment is maintained, which avoids the need for muscle reattachment and thus eliminates the necessity for postoperative immobilization.
References
1. Snapping Scapula Syndrome Meredith A. Lazar, Young W. Kwon and Andrew S. Rokito J Bone Joint Surg Am. 2009;91:2251-2262
2.Pearse EO, Bruguera J, Massoud SN, Sforza G, Copeland SA, Levy O.Arthroscopic management of the painful snapping scapula. Arthroscopy. 2006;22:755-61.
3. Pavlik A, Ang K, Coghlan J, Bell S. Arthroscopic treatment of painful snapping
of the scapula by using a new superior portal. Arthroscopy. 2003;19:608-12.
4.Bell SN, van Riet RP. Safe zone for arthroscopic resection of the superomedial scapular border in the treatment of snapping scapula syndrome. J Shoulder Elbow Surg. 2008;17:647-9.