Cuff Tear Arthropathy
Dr.Senthilvelan
Consultant Orthopaedic Surgeon
For queries Contact 9566222533/[email protected]
The rotator cuff muscles are:
1. Supraspinatus 2. Infraspinatus 3. Teres Minor 4. Subscapularis
The tendons of these muscle coalesce to form the rotator cuff. The muscles are inseparable at this level, except for subscapularis which is separate and joined to the rest of the cuff via the rotator interval.
Supraspinatus
Supraspinatus is not only an initiator of abduction, but acts throughout the range of abduction of the shoulder. It has equal abduction power as deltoid. Note that it lies in the scapular plane – i.e. 30 degrees to the coronal plane
Infraspinatus & Teres Minor
These two muscles lies below the scapular spine and are external rotators of the shoulder. Infraspinatus primarily acts with the arm in neutral and Teres Minor is more active with external rotation in 90 degrees of abduction.
Deltoid
The deltoid muscle is the only shoulder elevator if the supraspinatus is torn and dysfunctional. Therefore most rehabilitation is directed towards this muscle. It comprises anterior, middle and posterior portions which are more active depending on the direction of arm elevation.
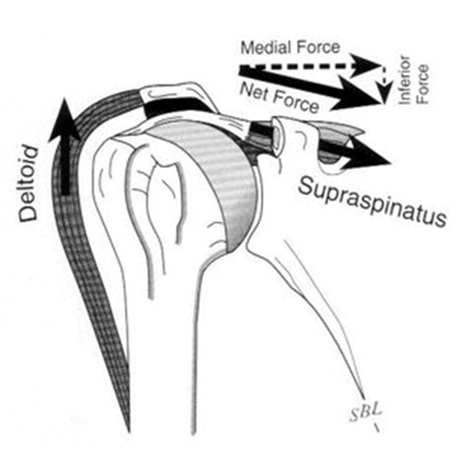
Force Couples
The rotator cuff muscles work together to contain the glenohumeral joint, which is an inherently unstable joint. As the arm is abducted the resultant joint reaction force is directed towards the Glenoid. This ‘compresses’ the humeral head against the Glenoid and improves the stability of the joint when the arm is abducted and overhead.
 |
| Diagram explaining Force couple of normal shoulder |
 |
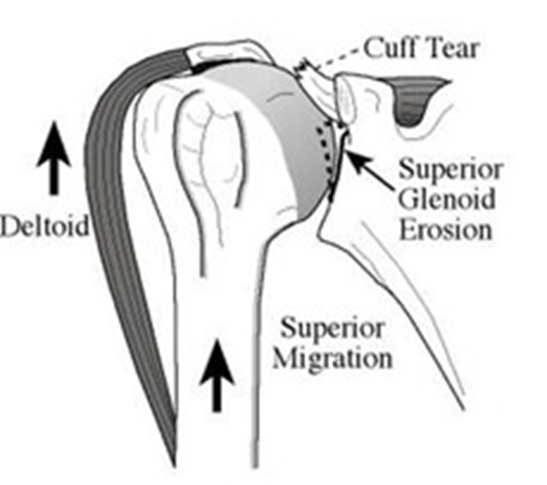
| Diagram explaining Force couple of Cuff tear arthropathy |
Cuff Tear Arthropathy
1977 that Charles Neer coined the term “cuff tear arthropathy.” Neer et al.went on to provide the first detailed description of CTA in 1983. CTA encompasses a condition characterized by a massive rotator cuff tear, proximal migration of the humerus resulting in femoralization of the humeral head and acetabularization of the acromion, glenoid erosion, loss of glenohumeral articular cartilage, osteoporosis of the humeral head and eventually humeral head collapse.
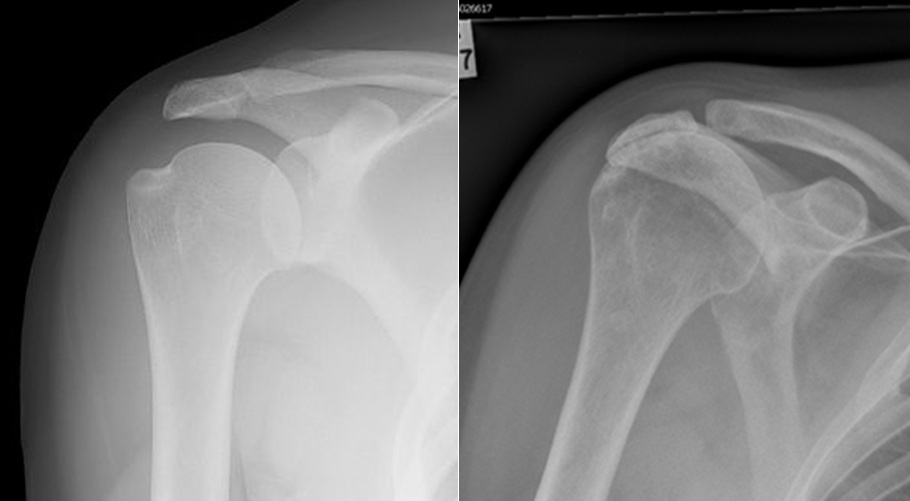 |
| Normal xrays on left compared to Cuff tear arthopathy on right. |
Radiographic Findings
Radiographs of the shoulder comprise an important step in the diagnosis and evaluation of CTA. Glenohumeral arthritis, osteopenia of the humeral head and superior migration of the humeral head, along with its sequelae, can be seen. Humeral migration leads to changes in the acromion, acromioclavicular joint, coracoid and glenoid. Abnormal contact between the humerus and the acromion can lead to rounding off of the greater tuberosity (femoralization) and concave erosion of the underside of the acromion (acetabularization).
 |
| 3D CT showing Cuff tear arthropathy |